|
|||||
|
|||||
Klimaka-Suicide Prevention helpline 1018
K. KATSADOROS
Abstract
During the years 1999-2009, 4042 suicides were recorded in Greece. Data analysis shows a certain increase in the last few years. Specifically, during 2007 the number of recorded deaths is 328 (268 men, 60 women), while during 2009 rises to 391 (333 men, 58 women). In 2009 the most common method of suicide was violent (hanging). The highest suicide rate for men was found in Ionian Islands, followed by East Macedonia/Thrace and Crete while for women the highest suicide rate was found in Southern Aegean, followed by Peloponnese and Crete. Klimaka operates the only Suicide Prevention Helpline in Greece, 1018, since 2007 under the auspices of the Greek Ministry of Health and Social Welfare, Mental Health Division. During 2010, the helpline received approximately 2500 calls. The operation of the suicide helpline 1018 is part of a broader attempt of the organization KLIMAKA which aims to prevent and face the problems of suicidality and self destructive behavior. Other than the line, the major axons of the program are psychiatric and psychological help of self destructive and suicidal people, interventions to raise awareness of the public, interventions to inform and motivate particular professional groups who can play an important role in the timely recognition of self destructive behavior, training of Mental Health professionals etc. Encephalos 2011, 48(4):151-158.
Key words: Suicide, prevention.
I. The way of operation
Klimaka operates the only Suicide Prevention Helpline in Greece, 1018, since 2007 under the auspices of the Greek Ministry of Health and Social Welfare, Mental Health Division. The line operates on a 24/7 base, accepting phone calls from all parts of the country, charging the callers just a local phone call fee. All phone calls are anonymous and confidential. The line is staffed by specially trained mental health professionals (psychiatrists and psychologists). Specifically, up to now, six psychiatrists, seven psychologists and a group of volunteers, consisting of psychologists and social workers, have been occupied on the line.The line is intended for people with suicidal ideation, former attempters, those who are concerned about someone else, those who have lost someone to suicide and those who just want to get informed about suicide and self destructive behavior.
The goal is the management of the self destructive crisis so as to make sure of avoiding the danger in the here and now and, additionally, to ensure that the callers and their families will receive both psychological and psychiatric help as needed.
For that reason, when appropriate, the scientific personnel of the organization stay in touch with the caller providing them mental health assistance. Callers who live far away from Klimaka’s outpatient treatment centers are referred to hospitals and clinics located nearby the caller’s area of living, staffed by government employed mental health professionals.
The whole program of suicide prevention does not consist of the suicide helpline alone; there are other parts of the program as well. These parts, mentioned extensively in the section “Axons of Intervention”, are complimentary to each other aiming to cover the immediate and long term needs of the suicidal caller (continuous communication with professionals, regular counseling sessions, short and long term assistance to the patient and their family. Unfortunately, these needs are not always covered by the national health system.
Review of the operation of the Helpline for the year 2010
During 2010, the help line received approximately 2500 calls not including wrong phone calls, silent calls and calls asking for information about the line which are more than 3.000 in total. The majority of the calls (77%) were from the person who suffered from suicidal ideation while the rest (23%) from another person (a relative, a friend, a colleague etc.)
Particularly, 40% of the callers did mention a past attempt while 75% were suffering from suicidal ideation. Furthermore, 33% had a serious suicidal ideation, meaning that they had a particular plan of how to commit suicide. Although the majority of the callers with suicidal ideation were women (58%), men were more represented in the group of callers with serious suicidal ideation (65%).
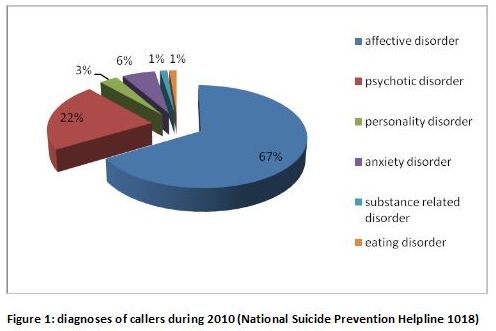
The majority of the callers were conducting a mental health professional for the first time. A smaller percentage (40%) mentioned that they had received mental health services in the past and had a specific diagnosis. The majority of those suffered from an affective disorder (67%) usually depression, 22% suffered from a psychotic disorder and 6% from an anxiety disorder (figure1).
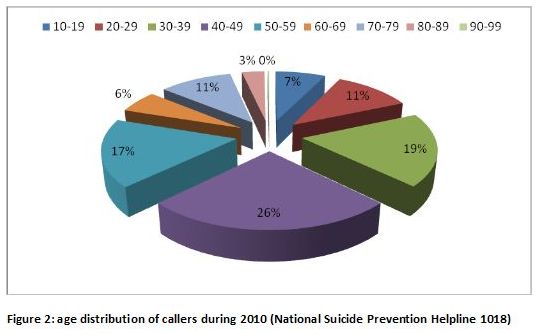
The majority of the callers were 40-49 y.o. (26%), the second most represented group was 30-39 y.o. (19%). The exact division in age groups is depicted in the following chart (figure 2).
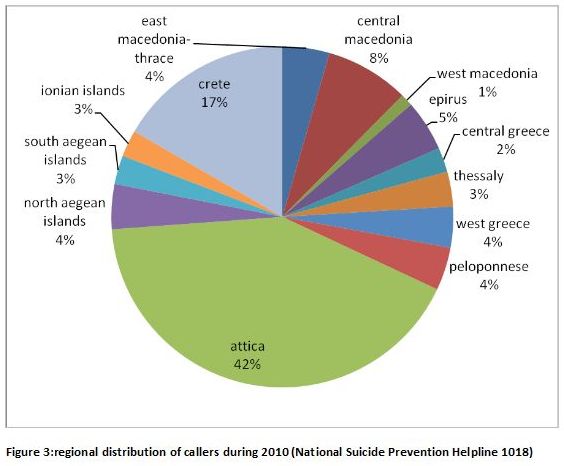
When it comes down to the specific geographic area of the country callers called from, the majority was from Attica (42%), second was Crete (17%), and third was the area of Central Macedonia (8%).
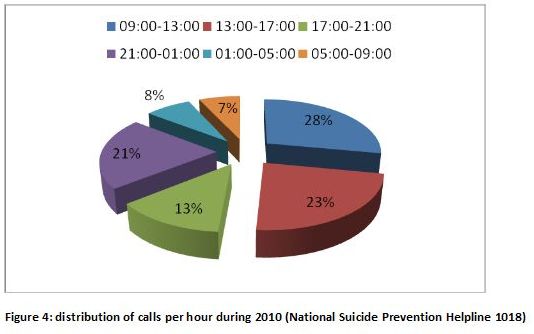
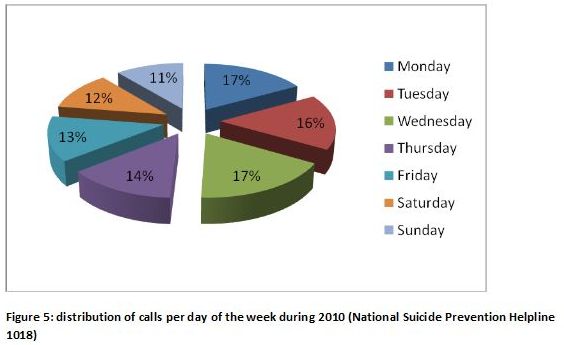
Time wise, 36% of the calls were between 9 p.m. to 9 a.m., while weekends account for the 23 % of the total (figure 4 and 5).
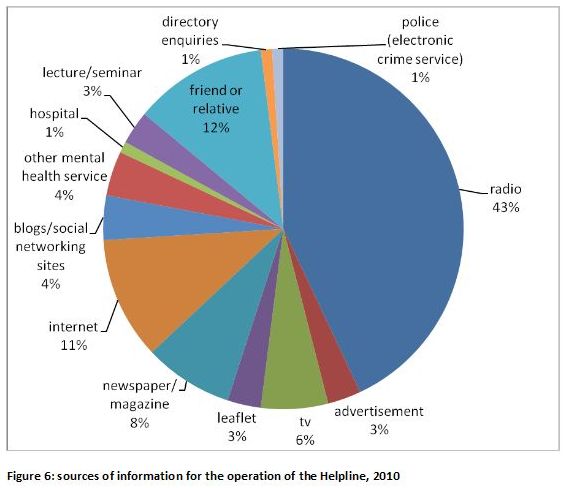
Callers learned about the help line from: radio 43%, from a friend or relative 12%, from the internet 11% while 4% of the phone calls were conducted by internet social media users and bloggers who informed us about posts that mentioned suicidal intention (figure 6).
II. Axons of Intervention
The operation of the suicide helpline 1018 is part of a broader attempt of the organization KLIMAKA which aims to prevent and face the problems of suicidality and self destructive behavior. Other than the line, the major axons of the program are:
1. Psychiatric and psychological help of self destructive and suicidal people
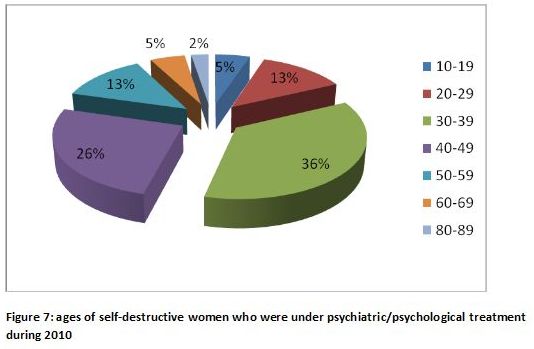
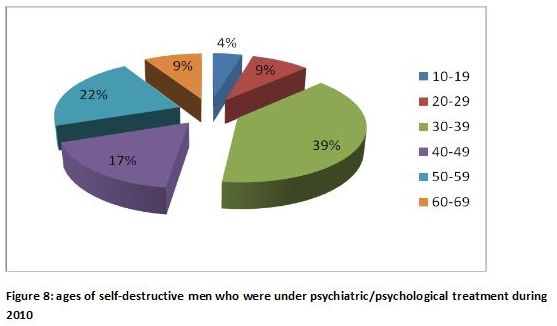
During 2010, 140 people were under psychiatric and/or psychological treatment by the scientific personnel of the Klimaka. The proportion of men and women was 66% and 34% respectively. The majority of both women (36%) and men (39%) were in the age group between 30-39 y.o. (figures 7 and 8), while the most common diagnosis was affective disorder (61%) (figure 9).
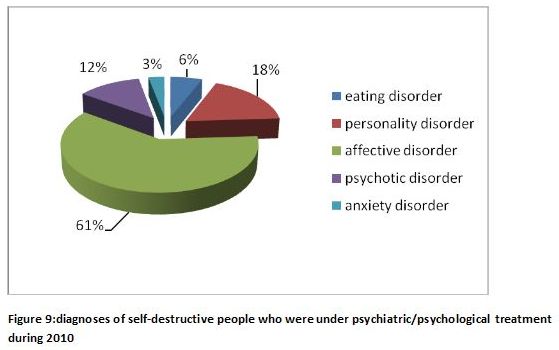
It is worth mentioning that two of the patients died by suicide. They were both men, could not be classified on Axon I of D.S.M. IV-TR, were suffering from personality disorders and had no supporting environment. They were both reffered to a psychiatric hospital but they were not accepted for treatment.
2. Interventions to raise awareness of the public (public speeches symposiums, fliers and leaflets)
Within that frame, people from Klimaka have delivered public speeches, organized special days, circulated fliers and leaflets and gave interviews in electronic means and the press so as to raise awareness about the problem.
3. Interventions to inform and motivate particular professional groups
These interventions aim professionals who can play an important role in the timely recognition of self destructive behavior by linking people at risk with mental health services. There have been seminars, speeches and symposiums while there have been written and circulated prevention guides to educators, doctors, nurses and people who work in the correction system.
4. Training of mental health professionals
In the years 2009-2011 three specialized seminars have been conducted in Athens. The duration of them varied between 24 to 33 training hours; 60 % of the program was theory and 40% experiential learning. In total, 56 professionals were trained: 32 psychologists, 11 social workers, 3 medical doctors, 3 psychiatric nurses, 1 sociologist, 1 educator and 2 general duty psychiatric rehabilitation workers.
Similar seminars have been offered to Patra and South Eastern Cyclades through Telepsychiatry while it is being planned to be repeated in Thessaloniki and Larissa.
Parallely to the training of mental health professionals, the department of social work of Klimaka organizes a web of social work services, amongst the municipalities and the hospitals of Athens and the rest of the country, in order to inform them about Klimaka’s program of suicide.
5. Creation of a web to promote cooperation amongst similar organizations both in Greece and abroad
Klimaka cooperates with:
While, since 2009, is a member of I.A.S.P. (International Association for Suicide Prevention).
6. Research and scientific publications about suicide and self destructive behavior
Klimaka analyzes the official data of the National Statistical Agency, about suicide, which cover the period 1980-2009. Data analysis and their statistical correlation with Greek sociodemographic variables is part of the research conducted by the scientific personnel of the organization.
7. Epidemiology of suicide worldwide
Suicide is a worldwide public health problem on the rise. According to the World Health Organization one million people die by suicide globally; more than those who die at war. This number means one suicide every 40 seconds, while the number of the attempts is fifteen to twenty times higher1.
During 2009 most suicides were recorded in China (170000), India (105000) and Russia (55000). However, the highest death rates were recorded in Lithuania (42.1 suicides per 100.000 people), Russia (38.7 per 100.000), Belarus (35.1 per 100.000)2.
According to Eurostat, in the European Union, during 2008, the average suicide rate was 10.1 suicides per 100.000 (for the 27 member states). The highest rate was that of Lithuania (30.7 per 100.000) while the lowest was that of Greece (2.8 per 100.000).
Epidemiology of suicide in Greece: data for 2009
During the years 1999-2009, 4042 suicides were recorded in Greece3. Data analysis shows a certain increase in the last few years; specifically, during 2007 the number of recorded deaths is 328 (268 men, 60 women), during 2008 rises to 373 (308 men, 65 women) and during 2009 rises even more to 391 (333 men, 58 women).
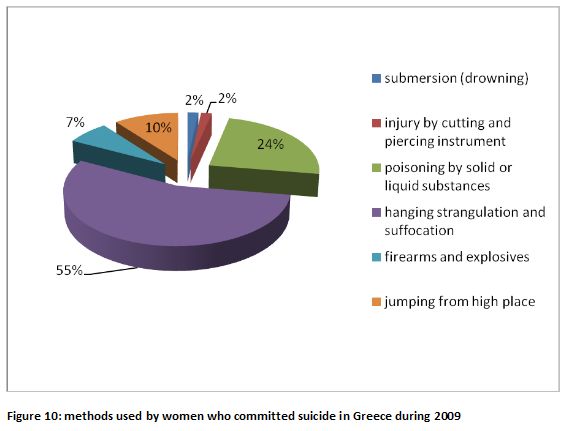
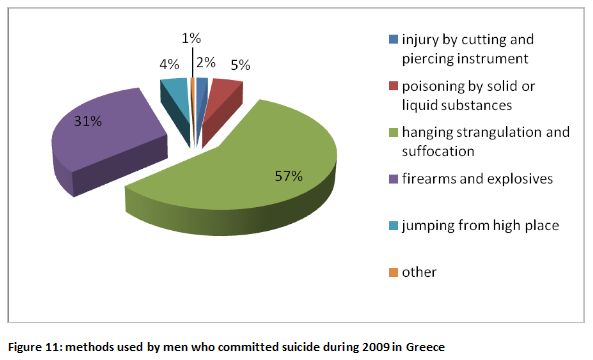
Data show that the methods are as follows: in 2009 the majority died by hanging (57% of men, 55% of women). Second most common method for men was shooting by a fire arm (31%) while for women was poisoning (24%) (figures 10 and 11).
Numerically, the majority of suicides were committed in Attica (108 men, 14 women) and in Central Macedonia (42 men, 9 women). In these areas resides the majority of Greek population.
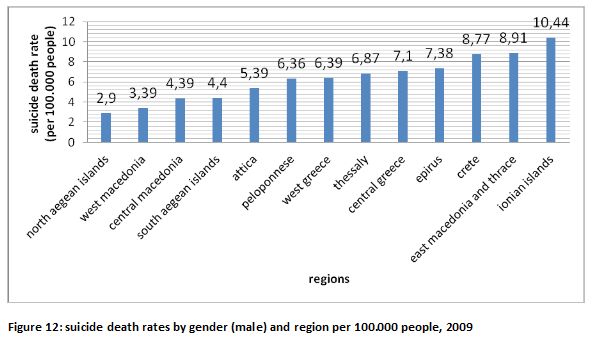
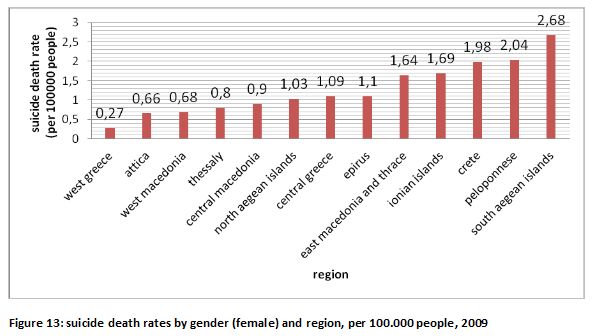
However the highest suicide rate for men was found in Ionian Islands (10.44 per 100.000), followed by East Macedonia/Thrace (8.91 per 100.000) and Crete (8.77 per 100.000) while for women the highest suicide rate was found in Southern Aegean (2.68 per 100.000), followed by Peloponnese (2.04 per 100.000) and Crete (1.98 per 100.000) (figures 12 and 13).
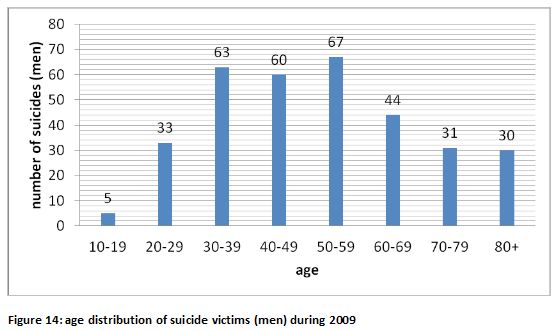
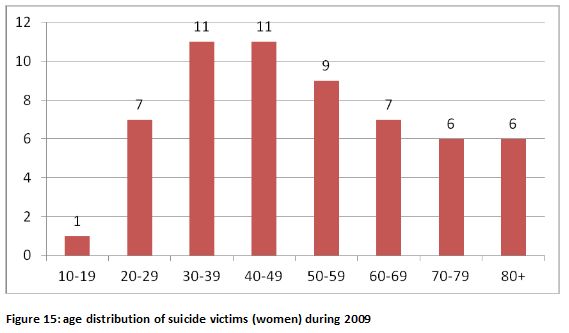
Most recorded deaths about men were in the age group 50-59 y.o. (67) while for women in the age group 30-39 (11) and 40-49 (11) (figures 14 and 15).
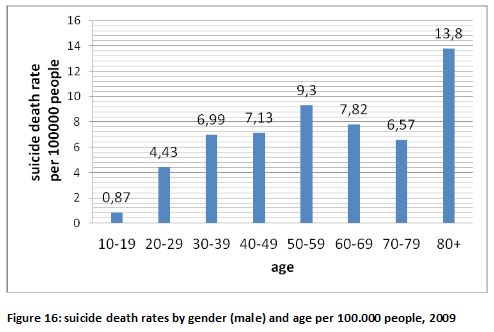
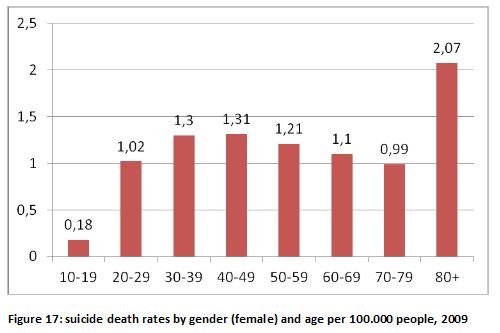
However, the highest suicide death rates for both men and women were in the age group of people over 80 (13.8 per 100.000 for men, 2.1 per 100.000 for women) (figures 16 and 17).
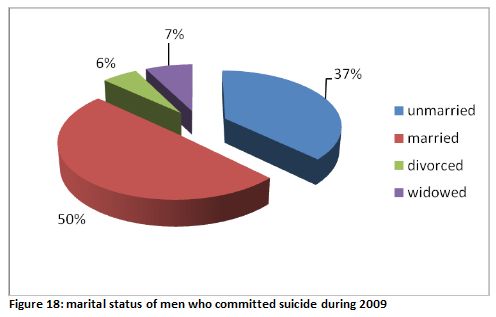
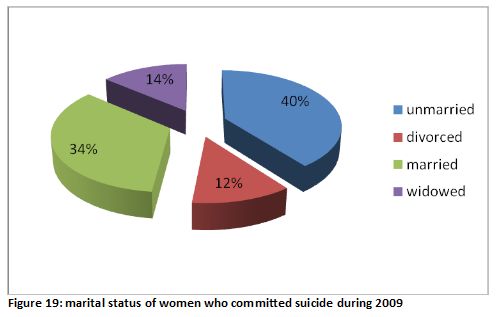
The majority of women who committed suicide during 2009 were unmarried (23 subjects, 40%) while most men were married (165 subjects, 50%) (figures 18 and 19).
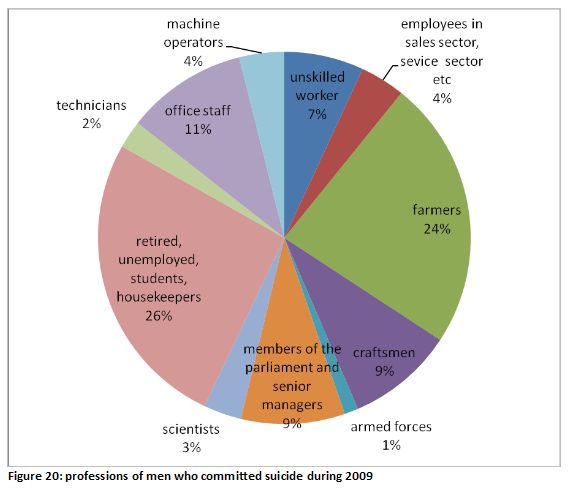
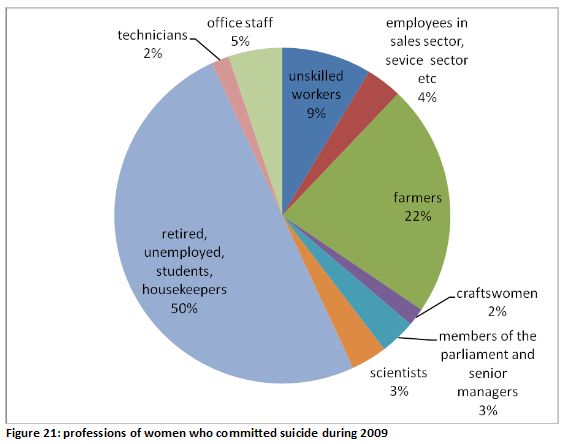
For both men and women the majority of suicides were committed by unemployed people (retired, unemployed, students and housekeepers). As for those who belonged to the work force the work group with the highest percentage was the farmers (24% of men and 22% of women). (figures 20 and 21).
Concluding, we want to emphasize that the problem needs to be studied extensively so as to create a national strategy for suicide prevention appropriate for our country.
1World Health Organization, www.who.int
2Wasserman D., “Oxford Textbook of suicidology and suicide prevention. A Global Perspective”, 2009
3National Statistical Agency,www.statistics.gr
